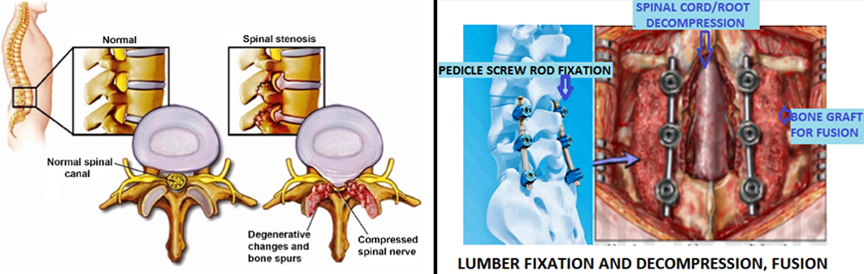
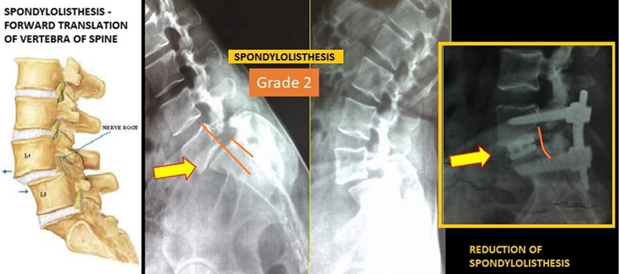
Lumber stenosis and spondylolisthesis is developed due to age related degeneration. In Lumber canal stenosis, space available for spinal root and cord decreased and compression of neural tissue developed. Patient with lumber canal stenosis has NEUROLOGICAL CLAUDICATION -Pain /numbness/ heaviness in both lower-limb developed after walking of some distance OR on standing only. They may also associated with degenerative back pain. Spondylolisthesis means translation of one vertebra over other. This translation may developed with weakness of bone/facet joint resulted from congenital/developmental changes, degenerative changes, rarely traumatic. Patient with lumber spondylolisthesis has MECHANICAL back pain in addition to neurological claudication and radicular leg pain, weakness in foot.
Management : Conservative- non operative treatment(like medicine, injection, physiotherapy etc.) would give short duration of symptom relief and tried for early and non complicated cases. Common type of surgical option available for each as below.
For Lumber canal stenosis
- Decompression laminectomy – decompression of neural tissue with removal of some part of lamina/bone.
- Fixation and decompression – in sever spinal canal stenosis, fixation is required to avoid spinal instability in future and to avoid recurrence of pain/symptom
For Lumber spondylolisthesis SURGERY : REDUCTION–FIXATION–FUSION-DECOMPRESSION
- POSTERIOR PEDICLE SCREW ROD FIXATION-FUSION, DECOMPRESSION
- TLIF – TRANSFORAMINAL INTERBODY FUSION WITH PEDCLE SCREW FIXATION-FUSION,DECOMPRESSION (OPEN/MINIMALLY INVASIVE SURGERY)